

The images above show the ability of the Clear Passage®️ Approach to clear bowel obstructions without surgery. Noting the severe narrowing in the ‘Before’ images, the physician scheduled the patient for emergency surgery to remove and repair two obstructions in the intestine.
In the left images, we see “BEFORE” images of
- A six-inch long ‘string stricture’ as narrow as a coffee straw in the lower bowel, and
- An ‘hourglass obstruction’ severely restricts the upper bowel.
The patient requested Clear Passage therapy instead of surgery. Images AFTER Clear Passage’s hands-on treatment (only) show that our therapy cleared both obstructions – without surgery. The physician canceled the surgery as it was “no longer necessary.”
Stopping Repeat Obstructions with Natural Bowel Obstruction Treatments
In a series of ground-breaking studies, a hands-on physical therapy (Clear Passage® Approach) designed to reduce or eliminate adhesions has been shown to decrease recurring total SBO events by 15 times the norm – with just five days of therapy. Using no surgery and no medications, this treatment was shown to be safe and highly effective at reducing or eliminating adhesions and bowel obstructions.
Treating Recurring Bowel Obstructions:
What therapy is like:
Our treatment program generally consists of 20 hours of hands-on therapy designed to decrease the adhesions in your intestines and nearby areas. Treatment is often delivered in two-hour sessions, each morning and afternoon for five days. Patients are free to relax in their hotel or explore the local area between sessions.
Sometimes likened to deep, site-specific pressure, the therapy is specific to your specific adhesions – bonds that can form over years or decades. During your sessions, we will instruct you in self-treatment techniques to further clear your intestines of adhesions and to help you avoid future obstructions.
Complete our online Request Consultation form to receive a free phone consultation with an expert therapist and learn more.
Causes and Frequencies of Blocked Intestines
What Causes a Bowel Obstruction?
Despite the greatest education, training, skill, and compassion of any surgeon, internal scars called adhesions form as the body’s first step in healing from surgery. Unfortunately, post-surgical adhesions are widely regarded as the primary cause of bowel obstruction. Thus, the surgery that may save your life is often the cause of subsequent blockages.
Bowel obstructions (which people often refer to as blocked intestines) are usually due to internal scars (adhesions) that form in the small intestines (small bowel) and sometimes in the large intestine (colon). Adhesions form as the first step in healing from surgery, infection, inflammation, or trauma. Adhesions are a primary cause of obstruction or blockage in the bowel. Regardless of where they form, adhesions join structures with strong glue-like bonds that prevent organs from functioning properly.
Adhesions may form as curtains or ropes within or between the loops of the bowel, completely blocking the passage designed to transport food. When these adhesions prevent the body from processing food, a bowel obstruction can quickly become a life-threatening condition. In fact, bowel surgery was cited by the AMA as the second most common emergency room surgery in the USA. Adhesion removal is the fifth most common ER surgery.



Foods That Cause Bowel Obstruction
Certain foods, particularly those high in fiber or difficult to digest, can contribute to the risk of developing a bowel obstruction in individuals with underlying digestive issues or a history of gastrointestinal surgery. Foods such as nuts, seeds, corn, and raw vegetables are notorious for their potential to form indigestible masses, especially in cases where the bowel is already narrowed or compromised by conditions such as diverticulitis or prior adhesions. Ingesting large quantities of these foods without adequate hydration can lead to the formation of bezoars — hardened, indigestible masses that can block the intestines. Download Clear Passage’s FREE diet guide to help you avoid further bowel obstructions and learn about an SBO diet right for you!
Signs of a Bowel Blockage
Blocked bowel symptoms can include severe pain, nausea, or vomiting accompanied by difficulty or inability to pass gas or stool. Blocked from its normal clear passage, food becomes backed up. The intestines stop functioning, preventing the patient from eating or eliminating waste.
A more comprehensive list of bowel obstruction symptoms include:
- No bowel sounds
- Hyperactive bowel sounds
- Nausea and vomiting
- Stringy stools*
- Stomach cramps that come and go
- Diarrhea (if the bowel is partially blocked)
- Swelling or bloating of the stomach (distention)
- Pain or tenderness around or just below the belly button
- Constipation and the inability to pass gas (a sign of complete blockage)
*Stringy Stool
One of the lesser-known indicators of a bowel blockage is the appearance of a pencil-thin BM sometimes referred to as stringy stool. This symptom, often overlooked, suggests a partial obstruction, allowing only a narrow passage for stool to pass. The stringy consistency results from the stool being squeezed through the constricted section of the intestine, highlighting a change in bowel habits that warrants further investigation.
If you experience severe abdominal pain or other bowel obstruction symptoms, you should seek immediate medical care.
How Do You Clear Bowel Obstruction without Surgery: The Clear Passage® Wurn Technique
Clear Passage®️ has over three decades of experience decreasing the adhesions that cause obstructions without surgery. We have published studies in many peer-reviewed U.S. and international medical journals.
The Clear Passage® Approach is a very site-specific manual therapy, the result of decades of study and investigation by Clear Passage®️ staff. It is quite different from any other physical therapy that we know of. Like peeling apart the run in a three-dimensional sweater, this non-surgical technique focuses on reducing or eliminating adhesions, cross-link by cross-link (bond by bond).
This therapy has been credited with saving lives and returning normal lifestyles to many people, including those who suffer from recurring bowel obstructions. Clear Passage®️ therapists have had hundreds of successes decreasing or eliminating obstructions, and adhesions that block the intestines. We have broken the repetitive “adhesion-obstruction-surgery” cycle that many of their patients describe as their life before Clear Passage®️.
Other Small Bowel Obstruction Management
Once hospitalized with a bowel obstruction, the patient will generally have a nasogastric (NG) tube passed through the nose and into the stomach to relieve pressure. Physicians then place a PICC line into a vein to draw blood, and to give the patient nutrition, pain medications, etc. Then, the medical team will wait (sometimes for several days) to see if the obstruction clears on its own.
If the obstruction does not clear, patients generally must undergo surgery as the primary method to clear small bowel obstructions. While this surgery can save the lives of those in immediate danger, obstructions tend to recur for many patients as post-surgical adhesions form due to the very surgery performed to repair the bowel. Thus, many patients find themselves in a repeating cycle of “adhesions-obstruction-surgery-adhesions” with no end in sight.
Surgical lysis (destruction) of bowel adhesions major drawback due to the formation of new adhesions to repair the underlying tissue. Besides the creation of new scar tissue, the risks associated with general anesthesia.
A multi-decade study published in Digestive Surgery found that more than 90% of patients develop adhesions after open abdominal surgery and 55% to 100% of women develop adhesions following pelvic surgery. (Liakakos et al., 2001) Another study reported that 35% of all open abdominal or pelvic surgery patients were readmitted to the hospital more than twice to treat post-surgical adhesions during the 10 years after their original surgery. (Ellis et al., 1999) Thus, abdominal surgery has been identified as a major cause of adhesion formation, leaving many patients trapped in the “surgery-adhesions-surgery” cycle described earlier.
Published Studies and Success Rates – Clear Passage®️ Physical Therapy
To view a complete list of published success rates treating Bowel Obstructions with Clear Passage®️, please visit our Bowel Obstruction Success Rates page.
World Journal of Gastroenterology – 2018
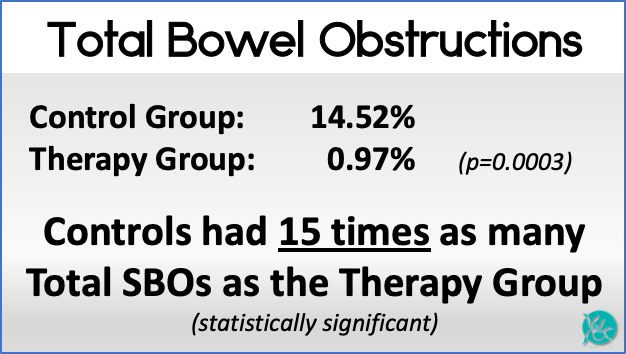
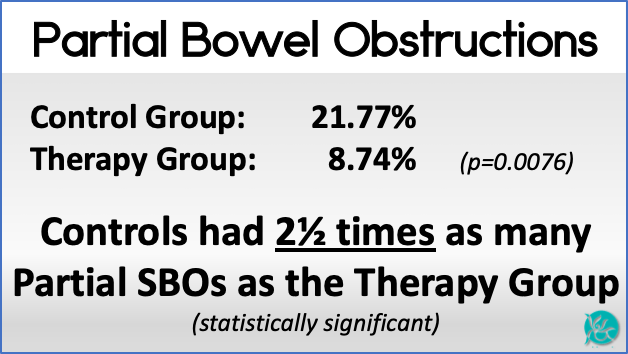
A large (Phase 2) controlled study authored by physicians from Harvard, Stanford, and Washington University medical schools examined repeat obstructions for patients who received the therapy vs. those who did not. Twenty hours of Clear Passage® therapy (often given over five days) decreased repeat bowel obstructions by several times the norm for patients who received the treatment vs. those who did not receive therapy. The results are shown below.
Clear Passage®️ therapists are experts at reducing adhesions and preventing bowel obstruction, without surgery.
Testimonials
To read previous patient success stories, please visit our testimonial page.
Dying from Bowel Obstruction
Bowel obstructions are a serious medical condition. Left untreated, they can lead to serious complications or death. The severity and potential fatality of a bowel obstruction depend largely on the cause, location, and duration of the obstruction, as well as the timely initiation of treatment. Without appropriate medical intervention, complications such as bowel perforation, sepsis, and severe dehydration can occur, significantly increasing the risk of mortality. Seek immediate medical attention if you are experiencing an obstruction. Treatment at Clear Passage® Therapies has been shown to decrease or stop further bowel obstructions and improve the quality of life!
Survival with Bowel Obstruction
Life dealing with reoccurring bowel obstruction is full of uncertainty, pain, and a decrease in function. Surgical intervention generally creates more scar tissue. Clear Passage® has been shown to decrease adhesions and clear bowel obstructions. When that happens, we find that pain and the fear of hospitalization for new obstructions decrease, followed by improved quality of life.
Related Content:
Research and Success Rates
- Study Results for a Non-Surgical Bowel Obstruction Treatment
- Study Results for a Non-Surgical Bowel Obstruction Treatment
- Bowel Obstruction Success Rates
Questions Answered
- Recurring Small Bowel Obstruction Treatment Frequently Asked Questions
- The Most Common Causes of Bowel Obstruction and How to Prevent It
- Bowel Blockage Symptoms
- How to Prevent Bowel Obstruction
- Can Diverticulitis Cause Bowel Obstruction?
- Seven Signs of Intestinal Blockage
- What to know before accepting an IBS Diagnosis
- How Long Does a Bowel Obstruction Last?
- What is the Cause of a Small Bowel Obstruction and What Are Your Options for Treatment?
- How Will My Lifestyle Change with Small Bowel Obstructions?
- Is There a Natural Treatment for Small Bowel Obstruction?
- What SBO Patients Can Expect From Treatment
Treatment
- At a Glance: Bowel Obstruction
- Bowel Obstruction
- Bowel Obstruction – Need Help Now?
- Bowel Obstruction Treatment
- [Infographic] The Main Causes of Bowel Obstructions
Patient’s Stories
- Bowel Obstruction: Patient Story Update
- Video Testimonial – A Mother’s Journey to Recovery: Small Bowel Obstruction
- What Is Bowel Obstruction? – A Patient’s Perspective
- A Glimpse into a Brave Young Boy’s Journey with CHARGE Syndrome
- Success Story: Clear Passage Allowed Me to Resume My Adventures
- Emergency Small Bowel Obstruction Surgery in India
- An End to Bowel Obstructions
Diet
- How to Relieve a Bowel Obstruction: Diet Guide
- Recipes For Bowel Obstruction Patients
- Diet Guide for Avoiding Bowel Obstruction
- Diet Modifications to Help You Handle a Small Bowel Obstruction
- Digestive Health Guide
- Bowel Obstruction: Diet & Lifestyle Recommendations
- Minimal Fiber Diet for Digestive Disorders
- Nutritional Guidelines
- Transitioning to a Regular Diet from a Low or Minimal Fiber Diet
- Low Fiber Diet for Digestive Disorders





